







Endometriosis Affects 1 in 10 Women. The Average Diagnosis Takes 7–10 Years.
A clinical overview of endometriosis — what it is, what it does, and why the persistent delay between symptom onset and diagnosis represents one of the most significant failures in women's healthcare today.
Endometriosis is a chronic, systemic inflammatory condition in which tissue resembling the endometrium — the lining of the uterus — grows outside the uterine cavity. It affects an estimated 190–200 million individuals worldwide, representing approximately 1 in 10 women and people who menstruate. Despite this prevalence, it remains one of the most underdiagnosed and poorly understood conditions in women's medicine.
March is Endometriosis Awareness Month — a global initiative coordinated by organisations including Endometriosis UK, the Endometriosis Foundation of America, and the Worldwide EndoMarch. The 2026 programme includes EndoFound's medical conference centred on the theme "Endometriosis 2026: A Nerve-Centric Disease" — reflecting the growing clinical focus on the neurological mechanisms that drive the condition's characteristic pain.
The average time from symptom onset to confirmed diagnosis is 7–10 years. This is not a measurement of diagnostic complexity — it is a measurement of how consistently period pain is normalised, dismissed, and misattributed. Endometriosis Awareness Month exists, in part, to correct that.
The Condition — A Clinical Definition
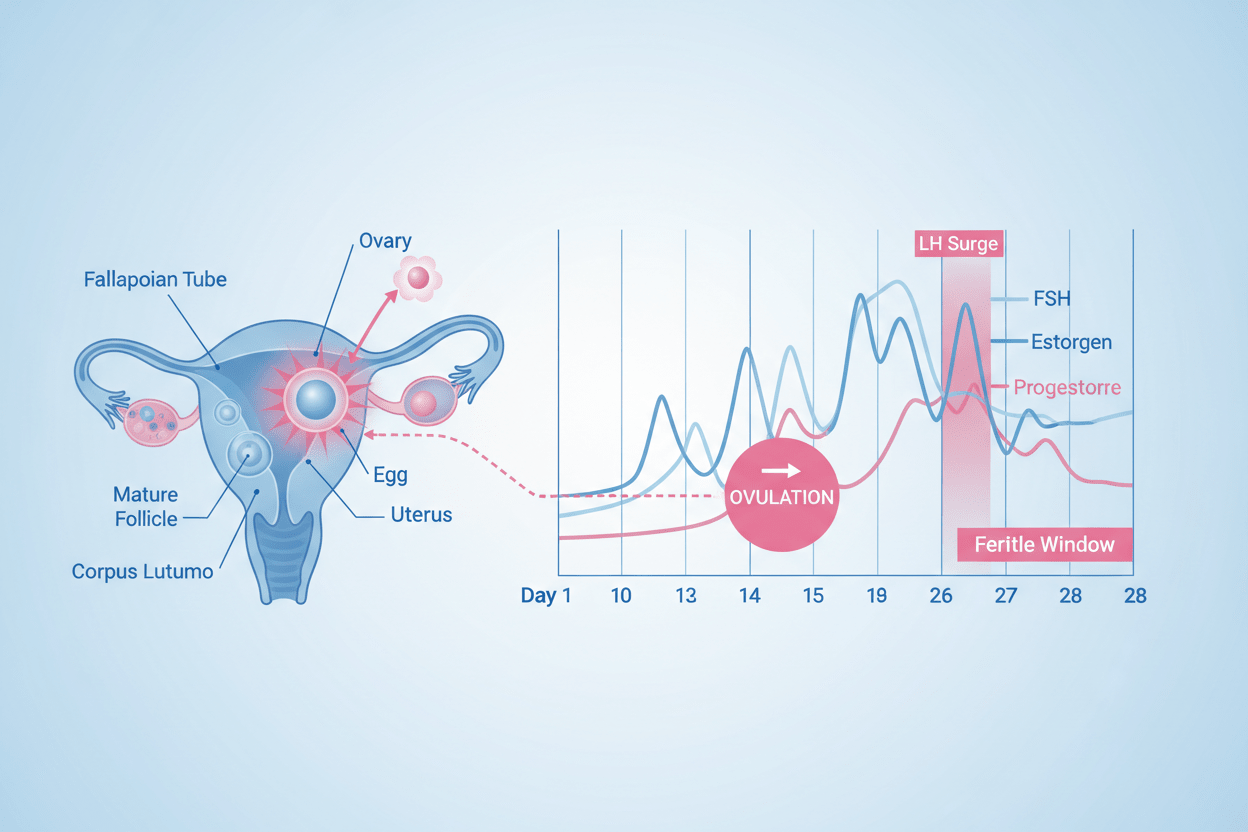
In endometriosis, tissue that behaves similarly to the endometrium establishes itself outside the uterus — most commonly on the ovaries, fallopian tubes, pelvic peritoneum, and bowel, though it can occur in more distant sites including the diaphragm and, rarely, the lungs (thoracic endometriosis).
This ectopic tissue responds to the same hormonal cycle as normal endometrium — thickening, breaking down, and bleeding with each cycle. Unlike normal endometrial tissue, however, it has no pathway to exit the body. The result is localised inflammation, the formation of adhesions (scar tissue that can bind organs together), and in the case of ovarian involvement, the development of endometriomas — blood-filled cysts sometimes called "chocolate cysts."
The precise aetiology of endometriosis remains incompletely understood. Leading theories include retrograde menstruation (in which menstrual tissue flows backwards through the fallopian tubes into the pelvic cavity), immune system dysfunction that fails to clear this ectopic tissue, genetic predisposition, and hormonal and environmental influences. It is increasingly understood as a systemic inflammatory disease rather than a purely gynaecological one.
Signs and Symptoms: What to Recognise
Symptom presentation varies widely. Some individuals experience severe, debilitating symptoms; others have minimal or no symptoms despite significant disease burden. Pain is the hallmark presentation — typically cyclical, worsening over time, and correlating with hormonal fluctuation.
Dysmenorrhea — Painful Periods
Severe pelvic cramping that begins before menstruation and persists for several days into the period. This is clinically distinct from typical menstrual discomfort — it is frequently debilitating, associated with lower back and abdominal pain, and unresponsive to standard over-the-counter analgesia.
Hallmark symptomChronic Pelvic Pain
Persistent pain in the lower abdomen, pelvis, or back occurring between periods or throughout the month — not exclusively tied to the menstrual cycle. This chronic pain profile is one of the features that most distinguishes endometriosis from primary dysmenorrhea.
Dyspareunia — Pain During or After Intercourse
Deep pelvic pain during or after sexual intercourse, typically caused by endometrial deposits in the pouch of Douglas or on the uterosacral ligaments. This symptom has a significant impact on intimate relationships and is frequently under-reported in clinical consultations.
Bowel and Urinary Symptoms
Pain on defaecation or urination, particularly during menstruation. Associated symptoms include bloating, constipation, diarrhoea, and in cases of bowel involvement, rectal bleeding. These symptoms frequently lead to misdiagnosis as IBS — a significant contributor to diagnostic delay.
Commonly misdiagnosed as IBSHeavy Menstrual Bleeding
Menorrhagia or irregular bleeding, including intermenstrual spotting. Excessive flow requiring frequent sanitary product changes is a clinically significant symptom that warrants investigation — not normalisation.
Fatigue
Profound, chronic fatigue — distinct from ordinary tiredness — is a frequently reported and significantly underacknowledged symptom of endometriosis. It is driven by a combination of systemic inflammation, chronic pain, disrupted sleep, and hormonal dysregulation.
Subfertility and Infertility
Endometriosis is identified in 30–50% of women investigated for infertility. The mechanisms are multifactorial — including anatomical distortion from adhesions, impaired ovarian reserve (particularly with endometriomas), altered hormonal environment, and inflammatory effects on egg and embryo quality.
Present in 30–50% of infertility casesThe Diagnostic Delay Is Not Inevitable
The 7–10 year average between symptom onset and confirmed diagnosis is driven by the normalisation of period pain, the misattribution of symptoms to conditions like IBS, and the historic underinvestment in women's pain research. Updated 2026 ACOG guidelines now emphasise earlier clinical diagnosis — beginning with transvaginal ultrasound as a first-line investigation — to reduce this delay.
Managing Endometriosis: Current Clinical Approaches
There is currently no cure for endometriosis. Treatment is individualised, typically multidisciplinary, and focused on symptom management, disease progression, fertility preservation where relevant, and quality of life. No single treatment is universally effective, and many patients require a combination of approaches over time.
Pain Management
NSAIDs (ibuprofen, naproxen) are the standard first-line pharmacological approach for pain reduction. For more severe cases, prescription analgesia may be required. Adjunct approaches include pelvic floor physiotherapy, acupuncture (with emerging evidence for pain reduction), and heat therapy.
Hormonal Treatments
Hormonal suppression — via combined contraceptives, progestin-only options (including the Mirena IUS, implant, or injection), or GnRH agonists and antagonists — reduces oestrogen levels to slow ectopic tissue growth and suppress menstruation. Effective for symptom control, but symptoms typically return on cessation and existing tissue is not removed.
Laparoscopic Excision Surgery
Surgical excision — the complete removal of endometriotic deposits — is the most effective intervention for long-term pain relief and fertility improvement. Expert consensus (including EndoFound guidance) favours excision over ablation for deeper disease. Recurrence is possible; many patients benefit from post-operative hormonal suppression.
Fertility-Focused Pathways
For those wishing to conceive, surgical clearance of endometriosis followed by natural conception attempts, ovulation induction, IUI, or IVF represents the standard clinical pathway. Early referral to a fertility specialist with endometriosis experience is recommended — particularly where endometriomas are present.
- Period pain that is not adequately controlled by standard over-the-counter pain relief
- Pain that interferes with work, school, or daily activities around menstruation
- Pelvic pain that persists outside of the menstrual period
- Pain during or after intercourse that is deep rather than superficial
- Bowel or urinary symptoms that worsen cyclically with menstruation
- Difficulty conceiving after 6–12 months of unprotected intercourse
If any of the above apply, seek assessment from a gynaecologist with experience in endometriosis. A clinical diagnosis can now be supported by transvaginal ultrasound as a first-line investigation, per updated 2026 ACOG guidelines — though laparoscopy remains the definitive diagnostic standard for many presentations.
This article is for informational and educational purposes only and does not constitute medical advice. If you are experiencing symptoms consistent with endometriosis, please consult a qualified healthcare professional.
Supporting Hormonal Health & Fertility, Whatever Your Journey Looks Like
Our HER FERTILITY formula is designed to support hormonal balance, cycle health, and reproductive wellbeing — as a complement to medical care, not a substitute for it. GMP-certified, evidence-based, and made in the UK.

{kind=link}
Leave a comment
All comments are moderated before being published.
This site is protected by hCaptcha and the hCaptcha Privacy Policy and Terms of Service apply.